
Graves’ Disease: What It Is, How It Works, And How To Support Your Body
If you have been diagnosed with Graves’ disease, or suspect your thyroid is involved in your symptoms, you are not alone. Graves’ disease is the most common cause of hyperthyroidism in iodine-sufficient regions, affecting roughly 1.3% of adults.
And like many endocrine conditions, it is surrounded by confusion, extremes, and oversimplified advice.
Some messaging frames Graves’ disease as purely a thyroid problem that can be “fixed” with medication alone. Other corners of the internet push restrictive diets, supplement stacks, or fear-based narratives about autoimmune disease. Neither approach reflects how the condition actually works in the body.
So let’s slow this down and get grounded.
This post is a clear, evidence-informed overview of what Graves’ disease is, how it affects your physiology, how it is diagnosed and treated, and how nutrition and lifestyle can support your body alongside medical care – without fear, hype, or false promises.
“Graves’ disease isn’t just a fast thyroid. It’s an immune-driven condition that affects multiple systems at once.”
What Is Graves’ Disease?
Graves’ disease is an autoimmune condition that causes hyperthyroidism. This means the thyroid produces excess thyroid hormone.
What makes Graves’ disease distinct is the mechanism.
In Graves’ disease, the immune system produces antibodies called TSH receptor antibodies (TRAb). These antibodies bind to the thyroid-stimulating hormone (TSH) receptor and stimulate it, essentially pressing the gas pedal on thyroid hormone production.
This is different from other causes of hyperthyroidism, such as thyroid nodules or thyroiditis, which are not autoimmune in origin.
Because of this immune-driven stimulation, Graves’ disease can also affect tissues outside the thyroid, particularly the eyes and skin.

What Distinguishes Graves’ Disease From Other Types of Hyperthyroidism?
Graves’ disease has several features that set it apart:
- TSH receptor autoimmune antibodies (TRAb) that directly stimulate thyroid hormone production
- Diffuse thyroid enlargement (goiter) rather than nodular growth
- Extrathyroidal manifestations, especially thyroid eye disease (Graves’ orbitopathy)
When thyroid eye disease is present, which include symptoms like eye bulging, dryness, grittiness, lid lag, or periorbital swelling, it is considered pathognomonic for Graves’ disease.
Other causes of hyperthyroidism may increase hormone levels, but they do not involve this immune-driven stimulation or the same pattern of systemic effects.
Common Symptoms (And Why They Happen)
Excess thyroid hormone accelerates metabolic processes throughout the body. This is why Graves’ disease often affects multiple systems at once.
Common symptoms include:
- Palpitations, tachycardia, or irregular heartbeat
- Weight loss despite normal or increased appetite
- Heat intolerance and excessive sweating
- Tremor and muscle weakness
- Anxiety, restlessness, and insomnia
- Diarrhea or frequent bowel movements
From a physiological perspective, this is not “anxiety out of nowhere.” Thyroid hormones increase sensitivity to catecholamines (like adrenaline), amplifying the stress response at a cellular level.
“Graves’ symptoms are not a lack of calm. They are a body stuck in overdrive.”
How Graves’ Disease Is Diagnosed
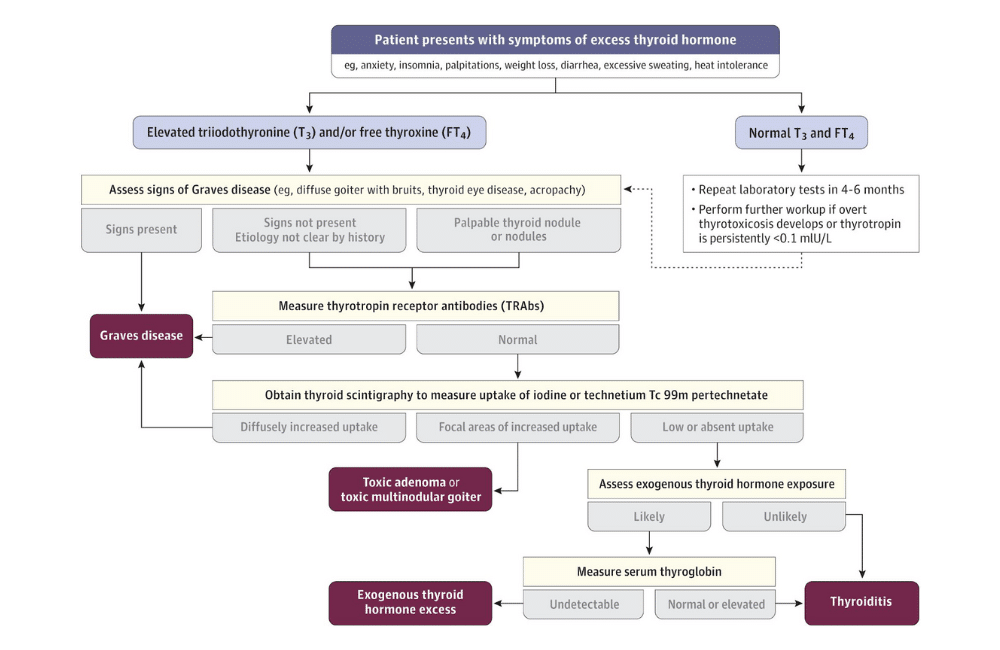
Laboratory Testing
The diagnostic process typically starts with a serum TSH measurement. TSH has high sensitivity for detecting thyrotoxicosis.
In Graves’ disease:
- TSH is suppressed (often <0.01 mIU/L)
- Free T4 and/or total T3 are elevated
Some individuals present with T3 thyrotoxicosis, where T3 is elevated and TSH is suppressed, but free T4 remains normal.
The most important confirmatory test is TSH receptor antibody (TRAb) testing. Modern immunoassays have sensitivity and specificity above 95%, making this the key diagnostic marker for Graves’ disease.
Imaging
When needed, thyroid imaging helps differentiate Graves’ disease from other causes of hyperthyroidism:
- Radioactive iodine uptake scans show diffusely increased uptake in Graves’ disease
- Thyroid ultrasound with Doppler shows increased vascularity, often described as a “thyroid inferno” pattern
Imaging is especially useful when antibody testing is inconclusive or radioactive iodine is contraindicated.

Treatment Options: What Actually Changes the Disease Course
Antithyroid Medications
Thionamides are the first-line treatment worldwide.
- Methimazole is the preferred medication in most cases
- Typical treatment duration is 12–18 months
- Propylthiouracil (PTU) is preferred during the first trimester of pregnancy
These medications reduce thyroid hormone synthesis but do not directly eliminate the autoimmune trigger. Relapse is possible after discontinuation, especially when TRAb levels remain elevated.
Beta-Blockers
Beta-blockers are commonly used early in treatment to reduce symptoms such as palpitations, tremor, and anxiety. They do not treat the underlying disease but provide meaningful symptomatic relief while thyroid levels normalize.
Definitive Therapies
When hyperthyroidism persists or recurs, definitive options may be considered:
- Radioactive iodine (RAI) is highly effective, but often results in hypothyroidism and may worsen thyroid eye disease, especially in smokers
- Total thyroidectomy is preferred in cases of large goiter, compressive symptoms, or when rapid control is needed
- Long-term low-dose methimazole is a safe and increasingly accepted alternative for some patients
“There is no single ‘right’ treatment, only the right strategy for your biology, symptoms, and life.”

Nutrition and Supplements: Supportive, Not Curative
Nutrition does not replace medical treatment for Graves’ disease; but, it plays a critical role in protecting your body during a hypermetabolic state.
Key Nutrition Priorities
- Adequate energy intake: Unintentional under-eating is common due to GI symptoms and anxiety
- Protein intake: Muscle breakdown increases during hyperthyroidism
- Calcium and vitamin D: Excess thyroid hormone accelerates bone turnover
- Iron and B12: Deficiencies are common and can worsen fatigue
Supplements to Use Carefully
- Biotin should be stopped at least 48 hours before thyroid labs, as it can interfere with results
- Iodine or potassium iodide should only be used under endocrinology supervision
More is not better here. Supplement strategies should be targeted, monitored, and clinically justified.
Lifestyle Factors That Matter More Than You Think
- Smoking cessation is one of the most important modifiable factors, especially for preventing or worsening thyroid eye disease
- Stress regulation matters – excess thyroid hormone amplifies the stress response, increasing nervous system load
- Sleep support is essential for immune regulation and symptom management
These are not “nice extras.” They directly influence disease expression and recovery capacity.
“Supporting the nervous system isn’t optional when the body is running hot.”

A Practical Meal Idea for Graves’ Disease Support
When metabolism is elevated, the goal is nourishment without overwhelm.
Balanced Snack or Light Meal Option:
- Greek yogurt or lactose-free yogurt
- Ground flax or chia seeds
- Blueberries or cherries
- Drizzle of honey or maple syrup
Why this works:
- Provides protein to support muscle tissue
- Supplies calcium for bone health
- Offers antioxidants without excessive fiber load
- Easy to digest when appetite or GI tolerance is low
Small, frequent meals like this often work better than large portions during active hyperthyroidism.

The Bottom Line
Graves’ disease is not just a thyroid issue. It is an immune-driven condition that accelerates metabolism, amplifies the stress response, and affects multiple organ systems at once.
Medication is essential. Nutrition, lifestyle, and nervous system support are protective. And long-term outcomes improve when care is thoughtful, individualized, and grounded in physiology.
The goal is not to “calm your thyroid” through restriction or fear-based strategies. The goal is to stabilize hormone levels while supporting the body systems under the most strain.
“That’s not alternative care. That’s complete care.”
Need support navigating Graves’ disease alongside medical treatment?
Our integrative dietitians help clients with hyperthyroidism and autoimmune thyroid conditions protect muscle, bone, and metabolic health while working alongside their endocrinology team so healing fits real life, not an idealized protocol.
MEDICAL DISCLAIMER
The information provided on this blog is for educational and informational purposes only and is not intended as a substitute for medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider, such as your physician, pediatrician, or a registered dietitian, before making any changes to your or your child’s diet, health routine, or treatment plan.
While we are a medical practice specializing in integrative and functional nutrition, the content shared here reflects general knowledge and holistic guidance, and may not be appropriate for every individual. Reliance on any information provided on this site is solely at your own risk.
REFERENCES
- Management of Graves Thyroidal and Extrathyroidal Disease: An Update. Kahaly GJ. The Journal of Clinical Endocrinology and Metabolism. 2020;105(12):dgaa646. doi:10.1210/clinem/dgaa646.
- Graves Disease: Latest Understanding of Pathogenesis and Treatment Options. Lanzolla G, Marinò M, Menconi F. Nature Reviews. Endocrinology. 2024;20(11):647-660. doi:10.1038/s41574-024-01016-5.
- Graves’ Disease. Davies TF, Andersen S, Latif R, et al. Nature Reviews. Disease Primers. 2020;6(1):52. doi:10.1038/s41572-020-0184-y.
- Hyperthyroidism: Diagnosis and Treatment. Mounsey A, Paulus R, Roten W. American Family Physician. 2025;112(2):146-152.
- Hyperthyroidism: A Review. Lee SY, Pearce EN. JAMA. 2023;330(15):1472-1483. doi:10.1001/jama.2023.19052.
- Hyperthyroidism: Aetiology, Pathogenesis, Diagnosis, Management, Complications, and Prognosis. Wiersinga WM, Poppe KG, Effraimidis G. The Lancet. Diabetes & Endocrinology. 2023;11(4):282-298. doi:10.1016/S2213-8587(23)00005-0.
- Hyperthyroidism. Chaker L, Cooper DS, Walsh JP, Peeters RP. Lancet (London, England). 2024;403(10428):768-780. doi:10.1016/S0140-6736(23)02016-0.
- Diagnostic Testing for Graves’ or Non-Graves’ Hyperthyroidism: A Comparison of Two Thyrotropin Receptor Antibody Immunoassays With Thyroid Scintigraphy and Ultrasonography. Scappaticcio L, Trimboli P, Keller F, et al. Clinical Endocrinology. 2020;92(2):169-178. doi:10.1111/cen.14130.
- Graves’ Disease in Clinical Perspective. Ehlers M, Schott M, Allelein S. Frontiers in Bioscience (Landmark Edition). 2019;24(1):35-47. doi:10.2741/4708.
